




Are you quite satisfied with his own body? If not satisfied, follow the advice of Margo Maine, Ph.D. following:
1. Your body is God's great, start to appreciate it.
2. Make a list that includes the things that your body can do. Read and add on the list.
3. Be aware of what your body can do each day. Remember that the body is the instrument of life, not just decoration
4. Make a list of people you admire: people who donate a lot of positive things in your life, in society and in the world. See if their physical appearance was important in supporting the success and accomplishments.
5. Walk with your head raised, supported self-confidence.
6. Do not let your weight or hinder your posture enjoy preferred activities.
7. Wear comfortable clothes, likes and feels good in the body.
8. Count the blessings you receive, rather than misfortunes.
9. Think of other things that can be achieved with time and energy spent worrying about weight and appearance.
10.Jadilah friend and supporter, not an enemy to his own body.
11.Pikirkan that regenerate your skin every month, every five days the stomach, liver every 6 weeks and bones every three months.
12.Setiap wake up in the morning do not forget to thank the rest for the body so the body feels fresh.
13.Setiap night when going to bed do not forget to tell your body how precious body, which helps carry out everyday tasks.
14.Temukan method of exercise that you enjoy and do regularly. But do not exercise to lose weight or against the body itself. Do sports for health and body strength, because it makes you comfortable.
15.Ingat back when you feel comfortable with your body. Tell yourself you can feel like that again, even at a young age that no longer.
16.Buatlah list 10 positive things about myself without mentioning physical appearance.
17.Buat writings and paste in the mirror: I look good from inside and outside.
18.Cari beautiful things in the world and yourself.
19.Mulailah said to myself: life is too short to spend hating their own bodies.
20.Makanlah when hungry and rest when tired. Find your friends can be reminiscent of the outer and inner beauty that is in you.
translate from http://kesehatan.kompas.com/read/xml/2010/01/01/18480434/20.cara.menghargai.tubuh.sendiri

20 How the Body Self-Respect
Personality in Medicine

Medicine is a profession which is closely linked to all of man's natural life, not only with the disease, medical knowledge and medical skill mastered. The ability to approach interpersonal empathic, understanding of life and human suffering as a whole, is a qualification that must be owned by a doctor into shape. Ability can not be generated only through a program of scientific medical education, but also requires the qualification and scope of the individual personality is conducive for medical education wrote it. Patients and families expect the precision, accuracy, speed, friendliness, safety, communication clarity, completeness, accessibility. The goal of medicine is to improve health, improve the overall meaning of life and to the quality of life better.
Reach the doctor patient relationship in terms of more complex interpersonal than social communication, 'employment contract' or 'commercial contract'. Meaning holy mission (sacred mission) which is based on professional expertise, sincerity, trust, caring and empathetic reply policy. The relationship is a human relations based on mutual trust that will try to help heal the patient.
Keywords that often appear in the doctor patient relationship is the acceptance (accepting the patient what it is), Empathy (the ability to understand and appreciate, not only cognitive aspects but also affective) and rapport (establishment of conditions of inter-personal relationships are emphatic, with an atmosphere of trust and understanding).
Being a good doctor, not a theory, IQ non-dependent, as well as academic ability. Not all doctors are able to behave / act ethical, professional and empathetic. Depending on the background of the personality, process development / experience of individuals, culture & environment, thought patterns, feelings / conscience, attitudes & behavior.
Understanding the behavior and personality
Human behavior gained from the study and instincts as animals. It is also influenced by biological, psychological education and social environment.
fungtional behavior expresion.Attitude is a way to bring themselves in social communication; mental status or feelings (eg, jealous attitude, low-self,) => expression of functional behavior. Behavior is typical of individuals in the act or respond to external and internal stimuli are expressed in the attitude and personality is based on trends. 'Conduct' is a general term, is more an act, based on ethical and moral considerations and a functional manifestation of personality (a reflection of personality). Personality - the individual characteristics indicate overall attitude, quality and variety of trends, character, behavior, emotions, that are unique to the individual. Developing lifelong and take shape (profile) which more or less settled in adulthood.
Not all personality patterns conducive to the field of medical profession that it needs to fit. Every profession has their own fitness. The style is not suitable as schizoid, obsessive (anankastik), paranoid, dependent, sosiopatik (anti-social, psychopathic), and so on.
Physician education also includes how to behave and berperilakuk as a doctor. Behavior can still be changed / redirected if there is a willingness to drive change, assisted by a conducive environment and the basic foundation of personality traits are not rigid. Adaptation is the ability Kondusivitas personality adjustment due to differences in cultural background and education, the adjustment towards the medical profession (the adjustment method of learning & teamwork, adjusting the view / philosophy of life), ability to tilikan and self-development capabilities. In terms of selection in pendidikanmeliputi institutions, clarity, consistency and consequences of various regulations (including sanctions), clarity of educational programs, campus atmosphere and role models as part of continuous learning.
Based on reference paper by
Prof. dr.Sasanto Wibisono, SpKJ (K)
Faculty of Medicine UI, Jakarta
Effective Communication
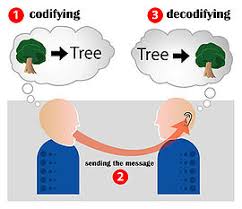
Communication is a process in which someone sends a message to others. The elements of communication include the news makers, news, media, news receiver, feedback, environment. A person who delivered the message usually want a change in the person receiving the message, either from simple things such as knowing something fact, until the occurrence of behavioral change. In connection with the patient's doctor for example, doctors wanted a change in the patient such as increased knowledge, change attitudes, to change behavior (taking medication regularly, diet or regular exercise). Said that effective communication when what you want to understand the provider submitted the recipient.
In the doctor patient relationship, effective communication is important to improve patient compliance, improve patient satisfaction, reduce malpractice claims and improve provider job satisfaction. Patients have the right to get information related to his problems, get the full treatment of attention and appreciation and express their opinions.
Include this level of communication is how I perceive me (the provider selfish), this how I perceive you (the provider listen to and observe the patient's behavior), this is how I perceive you seeing me and hearing me (the provider feeling the effects on the patient's words) , this is how I think you see me seeing you (there empathic communication, the provider understand the patient's situation at that time, communicate with the spirit and responsive to verbal speech and non-verbal patients behavior. When you understand these levels, the provider can anticipate the communication process, understand what is implied and the impact his words. To achieve a satisfactory result communication, communication skills required (interpersonal communication) to be trained every day and everywhere.
The steps in the communication is self-awareness (each communicating, always ready to practice the theory of interpersonal communication), realize that people who communicate with us may not know how to communicate well and practice it every day. This will help us become better communicators.
Interpersonal Communication (KIP) is the interaction between people with other people, two-way, verbal and non-verbal, sharing information and feelings with each other, or between individuals in small groups. These skills should have a doctor, namely verbal communication skills and non-verbal and verbal communication observation and non-verbal patients.
A. Verbal communication
(Communication through words spoken by someone)
a. Making patients feel comfortable
To make the patient feel comfortable, doctors need to be friendly, say hello, make connections (rapporting), making small talk with patients, explaining the authority and responsibility and client rights.
b. Ask questions
Doctors also have to ask and listen to patients to encourage clients to talk, show interest and attention to clients, increase our awareness of the feelings of the client, to obtain information and provide a referral to the client's conversation. From the questions we can be the general conditions, facts, feelings of clients and the reasons.
Questions can be grouped into open-ended questions that provide new opportunities for the emergence of various jaawaban and closed questions that only produce a "yes", "no" and the deeper questions raised when patients do not meet our need for such information. Closed questions are used to determine history of the disease. Open-ended questions to learn about feelings, beliefs and knowledge of the client. Deep questions to respond to client statements.
c. Active listening
Listening skills is to reflect the content of (paraphrasing), to reflect the feeling, and summarizing. Exchanging information shows that we care and attention. How do we talk and listen is as important as what we say. Must possess skills that are attention, concentration on the other person, summarize, reflect, do not cut, give non-verbal responses, and asked for an explanation.
Reflection Content (paraphrasing) is a reflection of the core speech has just been said by the patient. While reflecting feelings about the emotions of patients, and a core sense of feedback that the client is observed by the doctor. Emotions form the basis of most life experiences.
Paraphrasing involves the use of branch lines, key information used by patients to describe a situation or person, who pronounced the patient's core and accurately checks. While the reflection of feelings, the doctor imagine how the patient was feeling so communication and discussions went smoothly.
Summarizes almost like a reflection of the contents, the difference is to summarize the discussions conducted after some time and include some information submitted by the client.
d. Providing information
Information must be provided in simple language, honest, correct and complete.
e. Responding patients
In responding patients, there are some things to avoid, namely the verbal language is prohibited interrupt, criticize, assumptions and evaluation (do not believe the words of the patient. Meanwhile, in the non-verbal language for example, frowning, showing surprise or shock reaction, a smile that abusive (should show a neutral face).
In communicating, we are prohibited from assuming or evaluation. The assumption is too early to make conclusions, making conclusions without evidence (can not be inferred from the expression of verbal and non-verbal) of the things delivered by the patient. Evaluation is doubtful or put mistrust of what was said by the patient.
f. Encouraging patients to speak
Sometimes there are patients who are difficult to talk. Provider's duty to make them want to disclose the problem and provide enough information so that providers can establish the diagnosis and provide appropriate treatment.
B. Non-verbal communication
(all delivered by one person to another is not through words but through cues)
Communication vebal include non-voice (volume, speed, tone, vocals), face (gloomy, angry, smile, angry, disappointed), eye contact, gestures, body positions, and touch.
C. Observing verbal communication and non-verbal patients
Client's problem can be clearly known if the patient listens carefully, observing behavior (behavior) patients and ask questions effectively. Non-verbal observations made by observing the patient's face (sad, scared, confused, disappointed, down, angry, no eye contact, happy or satisfied) and the movements of the patient (anxiety, look at the clock again and again, hand made certain movements ). While in verbal language, observations were made on the verbal greeting clients if there is implied disappointment, anger, anxiety etc..
In communication there can be obstacles that interfere with. These barriers are factors such as recipient, the message, the message sender, the environment and the media.
RIGHTS OF FAMILY PLANNING CLIENTS
1. Information Rights: The right to know all the information relating to the issue of benefits and limitations dihadapinyamengenai tool / way of family planning.
2. Access Rights: The right to receive services regardless of gender, religion, creed, ethnicity, marital status and location.
3. Choosing the right: The right to decide freely in selecting and using family planning methods.
4. Rights Security / safety: The right to obtain services safe and effective
5. Privacy Rights: The right to privacy in counseling and family planning services.
6. Confidentiality Rights: The right to obtain assurance that the personal information provided will be kept confidential.
7. Rights Harkat Dignity; right to receive services in a humane, full of respect and attention.
8. Right Convenience: The right to comfort in the service
9. Rights Continuity: The right to a guaranteed availability of a tool / way family planning is complete and continuous service as long as necessary.
10. Right Thinking: The right to express opinions freely.
taken from handouts
Dr. Endang Basuki, dr, MPH
Departemen Ilmu Kedokteran Komunitas FKUI
Humanities in Medical Education: Some Contributions

Medicine is the most humane of sciences, the most empiric of arts, and the most scientific of humanities. (Pellegrino, 1970)
The human arts are the good arts of Aulus Gellus, the liberal arts, those that free a man’s mind from the tyranny of others. (Pellegrino, 1976)
The plan is to describe five ‘qualities of mind’ which are very important to medicine and which are distinctively contributed to by humanities in medical education. ‘Qualities of mind’ is meant to include items like ‘mind-set’, ‘attitude’, ‘awareness’. ‘perspective’, and ‘intellectual skills’. It is hard to make a case of such nebulous characteristics in a vocational school setting.
The ‘qualities of mind’ engendered by the humanistic disciplines, which will be described briefly, are: critical abilities, flexibility of perspectives, non-dogmatism, discernment of values, and empathy and self-knowledge. They are very similar to each other, bearing a distinct family resemblance.
In a medical school there seems to be an overwhelming amount of memorization, checklist, and cookbooks. This must be the most crippling, stupefying, and depressing feature of medical education to these bright and inquisitive young minds when they first arrive. And it never changes: the students simply adapt, they become molded.
Vocation learning that is task oriented must simply go on with what works, with what is immediately needed - whether it is a gadget, a business arrangement, a theory, or a therapy. The goal is clear - just learn the process and do it. By contrast, humanistic studies - art, philosophy, history, and literature - do not share this sense of immediacy.
Without the press of immediate practicality or pay-off, there is opportunity to play around with ideas - to seek, invent, try out, explain. This is the atmosphere in which imagination and critical thinking develop and flourish. In focusing on a work of art, a literary classic, a historic period, one can try out different interpretations, looking at it from different points of view.
‘Flexibility of perspectives’ is quite closely allied with ‘critical ability’ , yet different enough to be described separately. Professional education is often described as a kind of conceptual ghetto. Each profession has its own ghetto. Its members get locked in a certain way of seeing the world, themselves, their relationship with that world, and their role within it.
That may be what is meant by being ‘professionalized’. It is a way of viewing everything - certain things and relationships are highlighted, others fade into the background; certain causal chains predominate, others are barely noticed. In other words, one’s perspectives become highly specialized.
This is strengthened and reinforced throughout our professional education - by teaching, by emphasis, by exam, by the concepts we use daily, by our special language, by the handed-down view of what is significant. We get locked in. Our perceptions , thoughts, and lines of reasoning get channeled; our circuitry gets etched in.
‘Flexibility of perspectives’ is believed to be the most important contribution of the humanistic disciplines to medical education. The ability to quickly and easily shift perspectives when appropriate, to see with ‘new eyes’, is a valuable clinical as well as personal skill.
This ‘quality of mind’ bears close resemblance to the others and is nurtured by the same kind of intellectual exercises which train critical ability and flexibility of perspectives. Nothing promotes misguided certainty more than being locked into the kind of single perspective.
Seeing no alternatives, unable to imagine other possibilities, one becomes dead certain of whatever it is he is perceiving within the parameters and categories of his own limited vision. That is why flexibility of perspectives works as a corrective to incipient dogmatism.
But there are other ways to counteract it.
Through history, for example, we can come to know, understand, and appreciate a belief system other than our own. And when through history we see how frequently the unquestioned truth of a prior time were the falsehoods and myths of a later time, some doubts must inevitably be cast on those matters of current confidence.
We cannot help but be humble-struck, wondering what the next generation will do with things we are so cocksure of today. Particularly the history of science and medicine is helpful in this regard. We find gifted scientist being certain but wrong; we find unexamined assumptions; we find mistaken theories sometimes winning out; etc.
Through history our students gain a sense of discovery and of open-endedness of science. They acquire a mind-set ready to question, an openness to new clues, and a serious regard to recalcitrant data. In short, non-dogmatism.
Because this ‘quality of mind’ is probably the most obvious and frequent contribution of the humanities, it must here receive the most intense attention. In fact, with the enormous emphasis on biomedical ethics from the early 1970’s, it may seem downright commonplace. But values include far more than moral values.
They include others, such as political, aesthetic, and personal values, which tend to be overlooked in the intense concentration on moral values. The humanistic disciplines are heavily value-laden. But they are self-consciously so. They have the vocabulary, conceptual apparatus, and strategies for dealing with values.
Medicine, after all, is riddled with values. From its key concepts (disease, life, death, role of medicine, etc.) to diagnosis and therapy (what is ‘indicated’, trade-offs, lab values) to the delivery of health care (allocation, rationing, research-funding, etc.) medicine is value-laden. Not to identify these values is to be manipulated by them.
Empathy and self-knowledge, unlike the other qualities described, are more directed at interaction with persons than with observation, knowledge, and ideas.
Literature is probably the most direct way to illustrate this phenomenon. In literature we vicariously live many other lives. We are led by the writer’s skill to see life of others through a completely different mind-set.
Through such vicarious experience we surely learn about others in the most unique of all ways - by empathy, by ‘becoming’ them, by taking on so many of their characteristics that we begin to think, act, and react like them. We learn what it is like ‘to put ourselves in someone’s else’s place’, ‘to see it from the other person’s point of view’.
It is not only empathy and tolerance that flows from identifying with other persons, times, and beliefs. It is self-knowledge as well. We do not really know and understand ourselves until we see that, how, and why we differ from others. This, then, sets the agenda and motivation for self-investigation and reconstruction.
Prepared by
R. Sjamsuhidajat
Department of Medical Education, FKUI
excerpted from
“Humanities in Medical Education:
Some Contributions”
K. Danner Clouser (1990)
The Journal of Medicine and Philosophy 15:289-301
Please consider my friends's sites
-
-
Hello World7 years ago
-
UPDATE APLIKASI SAS 16.0.78 years ago
-
-
Komunitas Aeromodelling Dumai (KAD)12 years ago




